Alcohol Poisoning: Are Hospitals Releasing Drunk Patients Too Early?
A critical question in emergency medicine involves the potential dangers of premature discharge for patients suffering from acute alcohol poisoning. Intoxicated patients are usually brought to Emergency Departments for treatment, stabilization, and to confirm symptoms are solely from alcohol consumption. Consequently, blood alcohol concentrations (BAC) are typically determined. A pivotal study examined the characteristics of these patients and whether the admission BAC influences the critical decision to release them back into the community.
Table of Contents
- Key Characteristics of Patients with Alcohol Poisoning
- Discharge Decisions and Lingering Alcohol Poisoning Risks
- A Dangerous Precedent: Clinical Judgment Over Evidence
- Potential for Negligence in Alcohol Poisoning Cases
- The Critical Role of Forensic Toxicology
- Moving Towards Safer Discharge Protocols
- Alcohol Poisoning FAQs

Key Characteristics of Patients with Alcohol Poisoning
Between 2013 and 2014, 907 patients were admitted to a hospital Emergency Department in France due to acute alcohol poisoning. This represented 1.13% of all ED visits. BACs were recorded for 98.6% of these patients, with admission levels ranging from 0 to an extreme 0.600 g/100mL (median 0.250 g/100mL). A mere 2.7% of admission BACs were below 0.05 g/100m. Admissions peaked on weekends, with the busiest hours at 9:00 p.m. and 4:00 a.m.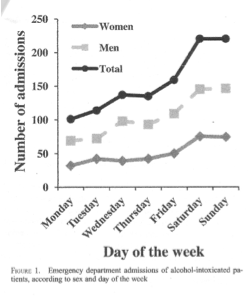
Patient demographics and details included:
- Ages ranged from 18 to 84 years (mean 37 years)
- The male to female ratio was 2:1
The mean length of stay in the ED was 19 hours (range 0 to 120 hours)
Discharge Decisions and Lingering Alcohol Poisoning Risks
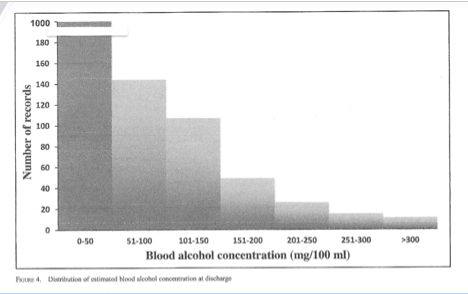
The study estimated the BAC at discharge using the time between admission and discharge and applying an average alcohol elimination rate of 0.015 g/100mL/h. The findings were alarming. Approximately one-third of the patients were discharged when their estimated BAC still exceeded France’s legal driving limit of 0.050 g/100mL. Even more concerning, some individuals were released with a BAC > 0.200 g/100mL, a level indicating severe intoxication and significant impairment.
A Dangerous Precedent: Clinical Judgment Over Evidence
This practice indicates that the decision to discharge a patient was often based on clinical signs of intoxication—such as slurred speech, unsteady gait, and bloodshot eyes—rather than the objective, reliable data provided by BAC and known alcohol kinetics. The authors state:
“We found that emergency physicians based the discharge decision on clinical judgment rather than on evidence-based medicine. The discharge decision may carry a risk of subsequent legal proceedings. The role of the accompanying persons must be defined and proof that the physician did everything possible to prevent the patient from driving after leaving the hospital, if estimated BAC is above the legal limit, must be recorded in the patient’s file. Allowing an unaccompanied patient to leave the hospital against medical advice is unadvisable, as the patient or a lawyer can always cast doubt on the quality of consent at the time the self-discharge form was signed.”
Potential for Negligence in Alcohol Poisoning Cases
The authors issued a stern warning regarding the legal and ethical ramifications of these discharge practices. They cautioned that if a patient discharged with a high BAC causes an accident, the attending physician could face serious charges. The study concludes that a physician could be charged with negligence if they failed to ensure the patient was accompanied upon discharge and was not a danger to themselves or others. This highlights a major gap in standard discharge protocols for cases of alcohol poisoning, prioritising convenience over comprehensive patient and public safety.
The Critical Role of Forensic Toxicology
Understanding the science of alcohol metabolism is paramount in these situations. Forensic toxicology provides the evidence-based framework that should guide medical decisions. Experts in the field, like forensic scientist James Wigmore, have spent decades refining the methodologies for BAC calculation and impairment assessment. Their work in courts and research labs provides the scientific backbone that can—and should—inform hospital policy to prevent premature discharge of vulnerable patients experiencing alcohol poisoning.
Moving Towards Safer Discharge Protocols
To mitigate these risks, hospitals must adopt more rigorous, evidence-based discharge protocols for intoxicated patients. This includes:
- Mandatory BAC testing at admission and before discharge.
- Using established alcohol elimination rates to estimate sobriety timelines.
- Requiring a responsible adult to accompany the patient upon release.
- Thoroughly documenting all discharge decisions and safety precautions taken.
- Providing clear educational resources to patients about the risks of driving impaired.
Implementing these steps can protect patients from harm, shield physicians from potential litigation, and ensure public safety is not compromised. The study serves as a crucial reminder that managing alcohol poisoning requires a blend of medical expertise and forensic precision.
Alcohol Poisoning FAQs
What is alcohol poisoning
Alcohol poisoning is a serious condition caused by consuming a large amount of alcohol in a short period, leading to dangerously high blood alcohol levels and potential life-threatening consequences.
Why are intoxicated patients brought to the Emergency Department?
Intoxicated patients are brought to the Emergency Department for medical treatment, stabilization, and to ensure their symptoms are solely due to alcohol consumption and not a hidden medical issue.
What did the study on alcohol poisoning and discharge decisions find?
The study found that emergency physicians often based discharge decisions on clinical judgment rather than blood alcohol concentration, leading to many patients being released while still legally impaired.
What was the highest blood alcohol concentration recorded in the study?
The highest admission blood alcohol concentration recorded in the study was an extreme 0.600 g/100mL.
How many patients were released with a BAC above the legal limit?
Approximately one-third of the patients in the study were discharged when their estimated blood alcohol concentration still exceeded the legal driving limit.
What are the clinical signs of alcohol intoxication?
Clinical signs of alcohol intoxication include slurred speech, an unsteady gait, and red, bloodshot eyes.
What is the average rate of alcohol elimination used in the study?
The study used an average alcohol elimination rate of 0.015 g/100mL per hour to estimate a patient's BAC at discharge.
What legal risk do physicians face when discharging intoxicated patients?
Physicians could be charged with negligence if a discharged patient with a high BAC causes an accident and the physician did not ensure the patient was accompanied.
What was the mean length of stay for intoxicated patients in the ED?
The mean length of stay for intoxicated patients in the Emergency Department was 19 hours.
What is evidence-based medicine in the context of alcohol poisoning?
In this context, evidence-based medicine refers to using objective data like blood alcohol concentration and known alcohol kinetics to make discharge decisions, rather than subjective clinical judgment alone.
Recent News

Impaired Driving Cases: Rats Don’t Drive
Impaired driving prosecutions require expert testimony grounded in human physiology, not animal studies. Occasionally humour...
Read More
The Three-Headed Hydra at Work: Which Drug Poses t...
Workplace injury prevention requires understanding which substances actually increase accident risk. The three most destructive...
Read More
Ethyl Alcohol Study: Top 80 Over 80 Research
Ethyl alcohol impairment takes centre stage in the groundbreaking “Top 80 Over 80” research from...
Read More
A Toxicology Definition Perspective: Does Gastric ...
Gastroesophageal Reflux Disease (GERD) is a digestive disease that occurs in approximately 10 to 20%...
Read More