A Toxicology Definition Perspective: Does Gastric Reflux Affect the Breath Alcohol Test Results?
Gastroesophageal Reflux Disease (GERD) is a digestive disease that occurs in approximately 10 to 20% of the population. Understanding its potential impact on forensic testing requires a clear toxicology definition perspective. “Reflux” means to flow back or return and refers to the flowing-back of the highly acidic stomach (gastric) contents into the esophagus.
A common symptom of this disease is heartburn. It is sometimes an issue in court, if the stomach contained alcohol from the consumption of an alcoholic beverage, could a reflux from the stomach affect the breath alcohol results? There have been a number of published studies about GERD and breath tests, but a recent study addresses this issue in 10 subjects with GERD using a high dose of alcohol.
Examining the Core Toxicology Definition in GERD Studies
Fifteen subjects, of which 10 were diagnosed with GERD, (5 male, 5 female ages 27 to 50 years) consumed a large dose of alcohol (1.7 g/kg for males and 1.5 g/kg for females) within 30 minutes. The alcohol was consumed after a standard meal of rice, beans, corn chips and spiced salsa. The subjects were tested under identical dosing conditions at least 3 weeks later to determine the reproducibility of the results, a key principle in scientific toxicology definition and analysis.
Blood samples were collected via a catheter every 20 minutes and BACs were measured by headspace GC. Breath tests were conducted at the same time as blood sampling in duplicate, using an Intoxilyzer model 5000. The rates of alcohol elimination ranged between 0.0103 and 0.0197 g/100mL/h which is consistent with previous studies. The mean rates of elimination were 0.0147 and 0.0159 g/100mL/h for the GERD and non-GERD subjects respectively.
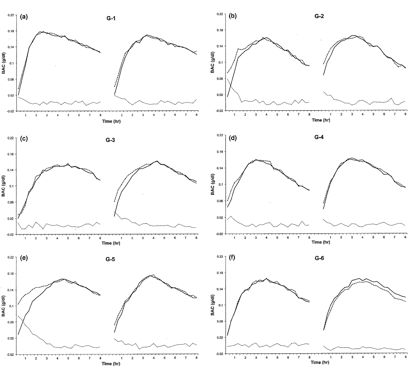
The following graph shows the BAC and BrAC curves of 6 GERD subjects (G-1 to G-6). The bottom curve shows when the BrAC is greater than the BAC, which in this experiment only occurred in GERD subjects shortly after drinking ceased, when there was a high alcohol concentration in the stomach.
Only 3 of the 10 GERD subjects produced elevated BrAC results that could be attributed to GERD and only 1 subject produced elevated BrACs on both drinking occasions. The authors conclude that GERD is not a factor to be considered when the subject is post-absorptive and only occurs when alcohol is present in the stomach at a very high concentration.
They also conclude: GERD-related alcohol leakage from the stomach into a breath sample is therefore an essentially irrelevant source of potential error in forensic breath testing. This conclusion is vital for legal professionals relying on an accurate toxicology definition of testing limitations.
Key Takeaways from the Research
- Incidence is Rare:Only 30% of GERD subjects in the study showed any effect, and it was not reproducible in most.
- Timing is Crucial:Effects occur only during the initial absorptive phase when alcohol is still in the stomach.
- Forensic Protocols are Effective:The standard observation period required before an evidential breath test, duplicate breath tests with good agreement, and the sloped detectors effectively eliminate this already rare issue.
- Post-Absorptive Phase is Secure:Once alcohol is fully absorbed into the bloodstream, GERD does not cause elevated breath test readings.
For other studies on GERD and the mouth alcohol effect check out my book – “Wigmore on Alcohol, Courtroom Alcohol Toxicology for the Medicolegal Professional”, Chapter 3.05 Mouth Alcohol, Irwin Law, 2011. This resource, penned by a recognised toxicology expert, provides an expanded toxicology definition of interference factors and is an essential tool for any medicolegal library.
The Role of Expert Toxicology in Legal Settings
The application of this science is where the theoretical toxicology definition meets practical legal defence. Forensic toxicology experts, such as those at Wigmore on Alcohol, interpret these complex studies for the courtroom. With extensive experience testifying in hundreds of cases, an expert can clarify that the Booker and Renfroe study confirms the reliability of breath alcohol testing in individuals with GERD, provided testing is conducted according to established forensic protocols.
This expert analysis ensures that courts can have confidence in the scientific evidence presented, understanding both its strengths and its validated limitations. The core toxicology definition of the testing process remains sound, and conditions like GERD, while a common concern, are shown by science to be a negligible factor in producing erroneous results.
Toxicology Definition FAQs
What is GERD?
GERD, or Gastroesophageal Reflux Disease, is a digestive disease where stomach contents flow back into the esophagus, affecting approximately 10 to 20% of the population.
Can GERD affect a breath alcohol test?
A definitive study concluded that GERD is an essentially irrelevant source of potential error in forensic breath testing, only potentially causing rare issues when alcohol is present in the stomach at a very high concentration immediately after drinking.
How many subjects with GERD showed elevated breath alcohol results in the study?
Only 3 out of the 10 GERD subjects in the study produced elevated breath alcohol concentrations that could be attributed to GERD.
When can GERD potentially affect a breath test?
GERD is only a potential factor shortly after drinking ceases when there is a high concentration of alcohol in the stomach; it is not a factor when the subject is post-absorptive.
What was the alcohol dose used in the referenced study?
In the study, males consumed 1.7 grams of alcohol per kilogram of body weight, and females consumed 1.5 grams per kilogram, consumed within 30 minutes after a standard meal.
How was alcohol concentration measured in the study?
Blood alcohol concentration was measured from blood samples collected via a catheter every 20 minutes using headspace gas chromatography. Breath alcohol concentration was measured in duplicate using an Intoxilyzer model 5000.
Were the elevated results easily reproducible in the study?
No, only 1 of the 10 GERD subjects produced elevated breath alcohol concentrations on both of the study's drinking occasions.
What is the toxicology definition perspective on this issue?
From a toxicology definition perspective, which is the study of the adverse effects of chemical substances, the research shows GERD has a minimal impact on the accuracy of forensic breath alcohol testing.
Where can I find more information on mouth alcohol effects?
For more studies, refer to the book "Wigmore on Alcohol, Courtroom Alcohol Toxicology for the Medicolegal Professional" by James Wigmore, specifically Chapter 3.05 on Mouth Alcohol.
What was the main conclusion of the Booker and Renfroe study?
The authors concluded that GERD-related alcohol leakage from the stomach is an essentially irrelevant source of potential error in forensic breath testing.
Recent News

Impaired Driving Cases: Rats Don’t Drive
Impaired driving prosecutions require expert testimony grounded in human physiology, not animal studies. Occasionally humour...
Read More
A Toxicology Definition Perspective: Does Gastric ...
Gastroesophageal Reflux Disease (GERD) is a digestive disease that occurs in approximately 10 to 20%...
Read More
Alcohol Poisoning: Are Hospitals Releasing Drunk P...
A critical question in emergency medicine involves the potential dangers of premature discharge for patients...
Read More
FVC and its Critical Relevance to Breathalyzer Tes...
An American criminal lawyer recently enquired about a female asthmatic client he had who was...
Read More